


Occipital skull reduction is a cosmetic cranial contouring procedure that reduces the prominence or projection of the back of the skull (the occipital bone). It is typically done for patients who feel the back of their head is overly protrusive, asymmetrical, or disproportionate in profile.


Common Reasons for the Procedure
- Prominent occipital “bump” or bulge
- Desire for a flatter or smoother skull contour
- Congenital skull shape concerns
- Residual contour irregularities after prior surgery or trauma
How the Surgery Is Done
The procedure usually involves:

- An incision placed within the hair-bearing scalp
- Exposure of the outer skull bone
- Burring/shaving down the outer table of the occipital bone using high-speed instruments
- Smoothing the contour for a more natural shape
- Closure of the scalp
The amount of reduction depends on:
- Thickness of the occipital bone
- Location of venous sinuses internally
- Desired aesthetic change
- Safety limits of the outer table removal
In some patients, only a few millimeters can be safely reduced; in others, more substantial contouring is possible.
Imaging
A CT scan with 2D or ideally 3D slicing is commonly used preoperatively to:

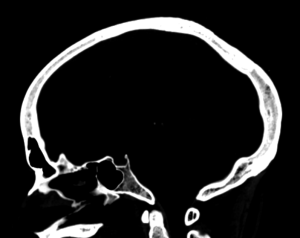
- Measure skull thickness (color mapping)
- Identify safe reduction zones
- Evaluate asymmetry
- Plan the contouring
Recovery
Typical recovery includes:
- Swelling for 1–3 weeks
- Temporary scalp numbness or tightness
- Return to normal activities in about 2 weeks
- Final contour settling over several months
Risks
Potential risks include:
- Scalp numbness
- Contour irregularities
- Hematoma or infection
- Visible scar (usually hidden in hair)
- Under-correction
Important Anatomical Limitation
Only the outer portion of the skull bone can generally be reduced safely. Internal cranial space and major venous structures limit how much projection can be removed.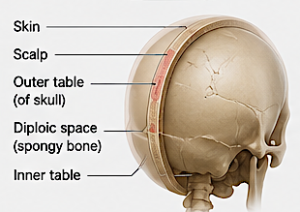
The realistic amount of occipital skull reduction is primarily determined by the thickness of the occipital bone and the location of the intracranial venous sinuses underneath it.
In most patients:
- Typical safe reduction: 5–8mm
- Good candidates with thick occipital bone: 10–12mm
- Rare exceptional cases: slightly more than 12mm in very localized areas
- Thin bone patients: sometimes only 2–4mm
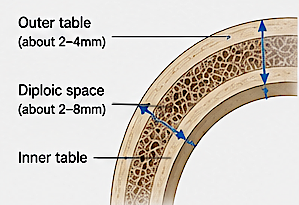
The key limitation is that only the outer table and diploic space of the skull can be safely reduced. The inner table of the skull cannot generally be violated.
A simplified way to think about it is:
Maximum Reduction?Outer Table Thickness+Diploic Space Thickness
Why CT Scans Matter
A 3D CT scan is essential because skull thickness varies dramatically:
- Central occipital bone is often thickest
- Areas near the transverse sinus become dangerous quickly
- Asymmetries are common
For example:
- One patient may have 14mm of bone thickness centrally and permit an 8–10mm reduction.
- Another may only have 6mm total thickness, limiting reduction to perhaps 3–4mm.
Aesthetic Reality
Even modest reductions can create noticeable profile improvement because the posterior skull silhouette changes substantially with a few millimeters of reduction.
A 6mm reduction may look visually significant from the side view and in short hairstyles.
Important Surgical Principle
The procedure is usually about:
- smoothing,
- flattening,
- and reshaping,
rather than dramatically shrinking the skull.
Patients seeking a “major size reduction” often overestimate what cranial bone surgery can safely accomplish.
When Larger Changes Are Possible
Larger apparent changes can sometimes be achieved by combining:
- occipital reduction,
- crown contouring,
- upper neck liposuction,
- hairstyle changes,
- or forehead/chin balancing procedures.
The overall head shape balance often matters more aesthetically than absolute millimeter reduction.
CT Scan Evaluation
Preoperative planning typically examines:
- Total bone thickness
- Outer vs inner table thickness
- Venous sinus location
- Skull curvature radius
- Distance from scalp to bone
- Symmetry
- Desired endpoint contour
The visual effect of occipital reduction is often larger than the raw millimeter number suggests because the eye perceives changes in the skull silhouette very strongly from side and oblique views.
3mm Reduction

A 3mm reduction is subtle but noticeable in the right patient.
Typical visual effect:
- Slight softening of a focal bump
- Less “pointed” posterior projection
- Mild improvement in side profile
- Usually most visible with short hair or shaved head
This amount is often appropriate for:
- mild asymmetry,
- small occipital knobs,
- or conservative contour smoothing.
Visually, it tends to look like:
“The bump is less sharp.”
rather than:
“The shape of the head changed.”
5–8mm Reduction
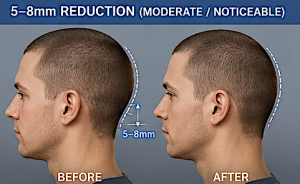
This is the range where most patients see a clearly appreciable aesthetic change.
Typical visual effect:
- Noticeably flatter posterior skull contour
- Reduced “bulbous” or “projecting” back-of-head appearance
- Better proportionality between forehead and occiput
- Significant improvement in profile photography
- Often enough to change hairstyle confidence
This is usually the “sweet spot”:
- meaningful change,
- while still remaining anatomically safe in many patients.
Most successful cosmetic occipital reductions fall in this range.
10–12mm Reduction

This is considered a large reduction and is only possible in select patients with thick occipital bone. But this amount of bone reduction is very rare.
Typical visual effect:
- Dramatic flattening of posterior projection
- Major change in side profile silhouette
- Can substantially alter overall head shape perception
- Often visible even with longer hair
However, there are important caveats:
- Not anatomically possible in many patients
- Greater risk of contour irregularities
- Larger scalp adaptation required
- Potentially more palpable bone thinning
Beyond ~10mm, surgeons must be extremely cautious about:
- entering thin bone,
- approaching venous sinuses,
- and creating unnatural flattening.
Why Small Numbers Matter So Much
The skull is a curved surface, so projection changes alter the entire contour arc.


A posterior prominence behaves visually somewhat like this:
![]() Flattening even a few millimeters changes the curvature over a much larger visible area.
Flattening even a few millimeters changes the curvature over a much larger visible area.
That is why:
- a 6mm reduction can look surprisingly significant,
- while patients sometimes incorrectly assume they need 20–30mm.
What Patients Usually Perceive
|
Reduction |
Typical Perception |
|
2–3mm |
“Softer/smoother” |
|
5–6mm |
“Noticeably flatter” |
|
7–8mm |
“Major cosmetic improvement” |
|
10–12mm |
“Significant head shape change” |
Another Important Reality
Photographs exaggerate occipital prominence:
- side lighting,
- shadows,
- hair compression,
- camera focal length,
- and head posture
all affect how prominent the occiput appears.
Patients frequently perceive their protrusion as larger than objective measurements show on CT.
Dr. Barry Eppley
Plastic Surgeon