


Background: The back of the head and concerns about its shape account for almost half of aesthetic skull reshaping patients in my experience. Concerns typical involve asymmetries from plagiocephaly, various types of occipital bone protrusions (knobs and buns) and flattening of part or all of the back of the head. The two techniques for back of head reshaping are one burring/shaving and implant augmentations. In the vast majority of cases only one skull shape problem exists which requires a single surgical technique.
But infrequently a combination of shape issues can affect one surface of the head. Most commonly in my experience it is the back of the head where this occurs because its overall shape is caused by the union of three skull bones, the solitary occipital and the paired parietal bones.
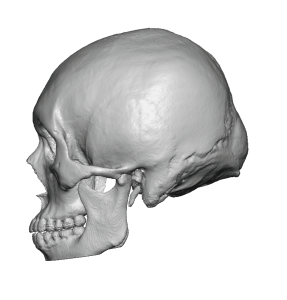
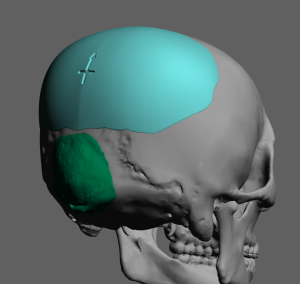
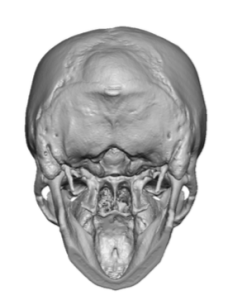 Case Study: This young male presented with back of the head shape concerns that consisted of a lower protrusion and and upper flat shape. A 3D CT scan shows a significant protrusion of the occipital bone (below the lambdoidal suture lines) and a flattened parietal area above it.
Case Study: This young male presented with back of the head shape concerns that consisted of a lower protrusion and and upper flat shape. A 3D CT scan shows a significant protrusion of the occipital bone (below the lambdoidal suture lines) and a flattened parietal area above it.
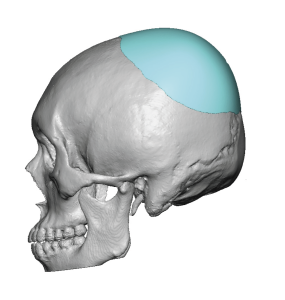
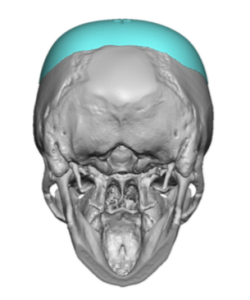 The approach to reshaping the back of his head consisted of a significant reduction of the protruding occipital bone (9mm reduction) with the placement of a custom skull implant above it. Total implant volume was 86ccs.
The approach to reshaping the back of his head consisted of a significant reduction of the protruding occipital bone (9mm reduction) with the placement of a custom skull implant above it. Total implant volume was 86ccs.

 Under general anesthesia and in the prone position a 7cm irregular zigzag scalp incision was made at the upper end of the occipital bone protrusion (and at the bottom end of the parietal flattening) through which the large occipital bone protrusion was reduced. A sequential approach was taken to the reduction, reducing it in segments to ensure an even reduction.
Under general anesthesia and in the prone position a 7cm irregular zigzag scalp incision was made at the upper end of the occipital bone protrusion (and at the bottom end of the parietal flattening) through which the large occipital bone protrusion was reduced. A sequential approach was taken to the reduction, reducing it in segments to ensure an even reduction.

 Once the occipital bone reduction was done the custom skull implant was introduced through the same incision but in a superior direction. Prior to its placement multiple through and through holes were placed through the implant with a dermal punch to allow for tissue ingrowth during the healing process.
Once the occipital bone reduction was done the custom skull implant was introduced through the same incision but in a superior direction. Prior to its placement multiple through and through holes were placed through the implant with a dermal punch to allow for tissue ingrowth during the healing process.

 Once in position (as seen through the bat-shaped scalp incision ) it was secured into position on the bone with two small titanium microscrews. The incision was closed with resorbable suture after the placement of a drain.
Once in position (as seen through the bat-shaped scalp incision ) it was secured into position on the bone with two small titanium microscrews. The incision was closed with resorbable suture after the placement of a drain.

 The immediate effect of the dual back of the head reshaping could be appreciated at the end of the surgery.
The immediate effect of the dual back of the head reshaping could be appreciated at the end of the surgery.

 At 48 hours after surgery the drain was removed and the upright change in the appearance of the back of the head mirrored what was seen during surgery.
At 48 hours after surgery the drain was removed and the upright change in the appearance of the back of the head mirrored what was seen during surgery.
 Tbe back of the head can be affected by numerous bone shape deformities. Bone overgrowths almost always in my experience involve the occipital or lower half of the back of the head. Bone shape deficiencies flat areas commonly affect the upper half of the back of the head or the parietal bone areas. While not typically seen together, when they occur the back of the head develops an unpleasing reversed slope shape. With an over developed occipital bone its reduction alone would have been aesthetically beneficial but building up the flatter top half of the back of the head provides the best aesthetic result.
Tbe back of the head can be affected by numerous bone shape deformities. Bone overgrowths almost always in my experience involve the occipital or lower half of the back of the head. Bone shape deficiencies flat areas commonly affect the upper half of the back of the head or the parietal bone areas. While not typically seen together, when they occur the back of the head develops an unpleasing reversed slope shape. With an over developed occipital bone its reduction alone would have been aesthetically beneficial but building up the flatter top half of the back of the head provides the best aesthetic result.
Case Highlights:
1) The back of the head can be affected by flattening and bony protrusion shape deformities…and in some rare patients both may occur simultaneously.
2) The occipital bone is prone to develop protrusions known as a bun while the upper back of the head (parietal bones) is prone to develop a flat area.
3) A 3D CT scan can accurately plan for an occipital bun reduction and a custom skull implant above it for a smooth and improved back of head shape in profile.
Dr. Barry Eppley
World Renowned Plastic Surgeon